PUNCTURE WOUNDS OF THE EQUINE FOOT, from THE ESSENTIAL HOOF BOOK, by Susan Kauffmann and Christina Cline
When it comes to puncture wounds of the hoof, some are obvious and easy to find, with the horse suddenly coming up lame and an examination of the foot turning up something sharp poking into the sole (fig 10.35). Unfortunately, we sometimes don’t know a horse has had a puncture in the foot until well after the fact. There may be no visible object to find, and the tract where penetration occurred often closes up quickly once the horse steps off or shakes loose whatever caused the injury. The problem with such “stealth” punctures is that any object that has penetrated into the foot can cause infection, and depending on what structures are involved, these infections can quickly become dangerous and very difficult to treat.

Finding a penetrating object in the foot is definitely alarming, but at least it gives you the chance to take appropriate measures right away. When a “stealth” puncture occurs without there being any way to really know it happened, that can sometimes end up being worse.
Deep puncture wounds are divided into three categories depending on where in the foot they are and what structures are affected. Type I wounds are located in the sole and may have caused damage to the solar corium and coffin bone. Type II wounds are found in the frog or heels, and because so many important structures are located just above the frog, these injuries can be extremely serious. Structures affected by type II puncture wounds may include the navicular bursa, the DDFT, the sheath of the digital flexor tendon, the impar ligament, the navicular bone, the coffin bone, the coffin joint, and the digital cushion. Type III injuries are less common and involve punctures of the coronary band. Damage from type III wounds may involve the coffin bone, collateral cartilages, or the coffin joint. All three types of wounds can easily become septic and cause catastrophic damage to the internal structures of the foot.

Deep puncture wounds in the heel or frog area can cause serious problems, as there are so many sensitive structures in this area of the foot. This horse was extremely lucky, as the deeply embedded nail managed to miss all of the critical structures.
If the infection walls off and forms an abscess, it is often very painful but not always a big problem. However, if the object has penetrated into any of the synovial structures located under the frog (e.g. the navicular bursa, coffin joint, or DDFT sheath), or into the bones of the foot, you have an extremely serious situation on your hands, as sepsis is a very real possibility. Infection in the interior structures of the foot can cause permanent damage that may result in irreversible lameness, and in some cases, the horse’s pain is so bad that euthanasia is the only humane option.
The best way to try to prevent a puncture wound from becoming a dire problem is to get your vet involved immediately. Even if the puncture looks minor, you should still call your vet, as infection can develop without any signs until the problem is well established. People often make the mistake of pulling out a penetrating object and thinking all is well because the horse seems better right away, then a few days later the horse goes lame and the foot is already septic. It is always better to be safe rather than sorry with puncture wounds, so get the vet on the phone as soon as possible and describe what you are seeing. If you can take pictures and send them to the vet right away, that will be helpful and will provide your vet with important information so that he or she can advise you on how to proceed.
When you find the horse with the penetrating object still in place, most vets will recommend that you not remove it, as they want a chance to examine it and possibly x-ray it while it is still in the foot. In some instances, they may want to perform an MRI to get a better look. Whether your vet wants to do x-rays or an MRI, diagnostic imaging is truly worthwhile when it comes to puncture wounds, as it allows the vet to see exactly where and how deep the object has penetrated, and whether or not any underlying structures are involved.
If you are leaving a penetrating object in place until the vet comes, you should try to stabilize the object to prevent it from being pushed further into the foot. This can often be accomplished by wrapping the foot with some sort of bandaging but maintaining a space around the object. If the object is on the bottom of the foot, taping a roll of duct tape or something similar to the foot so that the object is in the center of the roll can work in some instances, though you may have to come up with some other creative solution.
![]()
The owner of this horse taped a roll of duct tape to the bottom of the foot, preventing the nail from being driven in deeper. The vet left the roll on during the x-ray process, so it is visible in the radiograph.
Keep the horse in a clean, dry area, and encourage him to remain as quiet as possible until help arrives. If the vet cannot get to you within an hour or so, or you think the object will get pushed in deeper if you leave it in place, it might be necessary to remove it. Again, getting photos to your vet would be the best way to get advice in this circumstance. If you do remove the object, draw a circle around the spot where it penetrated before you pull the thing out, as the tract may close up and be hard to find afterwards, especially if it is in the soft, elastic tissues of the frog. Try to make note of the angle of penetration (take pictures if possible), and make sure to keep the object to show the vet.
Should you see something that you suspect could be a puncture but there is no visible object in the wound, you should still call the vet and mark the spot you are seeing. As long as the vet can find the spot, it is often possible to use a sterile probe or contrast dye in conjunction with x-rays to figure out the depth and direction of the tract the object left behind. Keep in mind that punctures don’t always look like a hole; they may appear to be a crack or fissure, often black in color.
Oftentimes, however, there will be nothing to see on the foot itself, and the puncture will only be discovered through signs of pain and/or infection. These may include:
- Sudden onset of lameness which may be mild or severe. Sometimes, initial lameness will not last very long, but will return within a few days and likely continue to get worse. Wounds that have punctured through the corium or deeper are usually quite painful soon after the foot is injured.
- Gradual onset of lameness that gets progressively worse over several days, which in the case of puncture wounds is a sign that infection is developing.
- An increased digital pulse which may be stronger on the side of the leg where the wound is.
- Heat in the foot or around the coronet.
- Sensitivity to pressure applied to the sole, often only around the spot of injury early on, but this may spread to the whole sole as infection takes hold.
- Favoring part of the foot.
- Standing with the injured foot forward.
- Swelling in the lower limb above the foot.
Treatment for a puncture wound will depend on the scope of the problem. If no critical structures have been damaged, treatment is not particularly complicated and full recovery is highly likely. Your vet will thoroughly clean the surface area of the wound with antiseptic solution, and may perform additional procedures such as lavage, debridement(removing damaged or infected tissue), and opening of the wound to allow drainage. A tetanus injection will likely be administered, and the vet may take a sample from the wound to culture, as knowing what types of infectious organisms are present will help in the choice of antibiotics, should they be used.
The foot will then be covered to protect it the wound from contact with contaminants. A bandage covered with multiple layers of duct tape on the sole works well as long as you stay on top of it to make sure the duct tape isn’t wearing through. Other options include hoof boots over a wrapped foot, or removable “hospital plates” added to shoes. Bandages will likely need to be changed several times or more, depending on the length of time your vet wants the foot to stay protected.
When internal structures are involved, treatment is likely to be intensive – more so if sepsis has already set in. Surgery may be required to gain access to the area and clean out damaged and infected tissue, and powerful antibiotics will be necessary, likely for a long course. Prognosis will range from good to grim, as some parts of the foot are more likely to recover from infection than others. If the coffin joint or navicular bursa is involved, the prognosis will be guarded, but the earlier treatment begins, the better the outcome is likely to be.
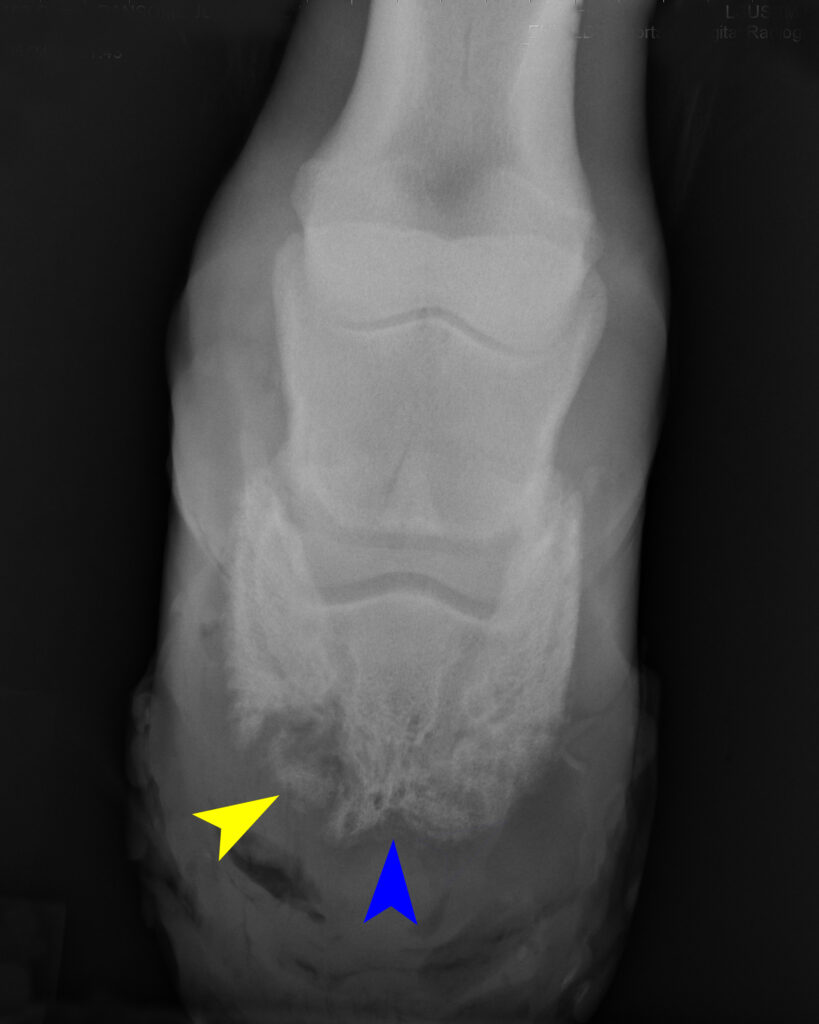
A puncture wound to this foot caused septic pedal osteitis, which resulted in bone loss that makes the solar margin of this coffin bone appear darker, ragged, and more porous (blue arrow) on an x-ray. The infection eating away at the bone has also caused a piece of bone to break off (yellow arrow). This sequestrum, as it is called, needs to be removed or it will cause chronic problems.
Wounds that do not appear to be healing will need further diagnostic imaging, as problems like septic pedal osteitis (infection of the solar margin of the coffin bone) and the formation of sequestrum (separated pieces of dead bone) can take weeks to show up (fig 10.40). When these problems occur, surgery is necessary to remove the necrotic bone tissue, but whether or not this is possible will be determined by what part of the bone has been affected and the extent of damage. If the bone is too far gone in a critical area, the horse may have to be put down.
Truly, any known or possible puncture wound should be evaluated by a veterinarian – not a farrier – as soon as possible, as only a vet can perform the diagnostic procedures and treatment necessary to keep a deep puncture wound from potentially becoming a disaster. Remember that a very dangerous wound might not look like much at all, so please, play it safe with foot punctures